Meniscus Tears
Updated 02/21/2015
Written and edited by Aruna Seneviratne, M.D
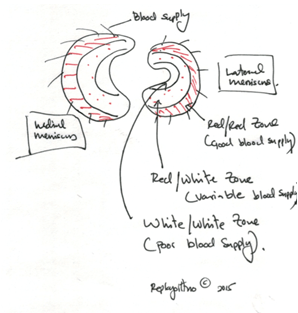
The meniscus is a C shaped piece of cartilage that resides between the two bones of the knee joint – the femur and the tibia. There are two menisci in each knee – one on the in-board side of the knee (medial meniscus), and one on the outboard side of the knee (lateral meniscus). They serve an important role in the function of the knee providing shock absorption, distribution of pressure, joint lubrication amongst other functions such as a secondary stabilizer of the knee.
Symptoms
Biology: Why does it occur?
Common Diagnostic Techniques
History: Diagnosing the problem begins with a detailed history that your surgeon will obtain from you.
Physical Exam: A thorough physical examination is conducted by your surgeon.
X-Rays: Plain radiographs (X-Rays) are the most important diagnostic study that is performed initially. For the knee your surgeon will obtain specialized views. Usually these are weight bearing x-rays – i.e.: you will be standing for the x-rays.
MRI: Your surgeon may obtain additional studies such as an MRI to look more closely at the meniscus and other soft tissues.
Treatment
Meniscus Surgery
The most common surgical treatment of meniscus tears is arthroscopic partial meniscectomy where a tiny camera is introduced into the knee via a tiny incision (keyhole surgery), and using arthroscopic instruments via a second keyhole, the torn piece of the meniscus is removed. The surgery takes about 20 minutes to complete and is performed under general anesthesia. This operation is one of the most common orthopedic operations performed in the United States.
Since the meniscus plays an important functional role in the knee, all attempts are made to preserve the meniscus and repair the tear if it is amenable to repair. Patient selection is important to ensure outstanding outcomes. Tears located in the vascular zone in younger patients are usually repaired. Dr. Seneviratne performs all three described techniques of repair – all inside arthroscopic repair, outside-in repair, and inside-out repair. Dr. Seneviratne has published techniques on meniscus repair.
Dr. Seneviratne will evaluate each patient individually and recommend a customized plan of surgical care.